


In May 2018, Yale University Medical School invited a select group of cardiologists, researchers, and health policy experts to discuss the controversial ORBITA trial in detail. Dr. Vikas Saini, president of the Lown Institute, and Shannon Brownlee, senior vice president, gave remarks about the historical context and implications of ORBITA; their edited remarks have now been published on the Health Affairs blog.
In his piece, Dr. Saini argues that by labeling stents as “ineffective,” we’re missing a key point of the ORBITA trial – the impressive power of medical therapy. The ORBITA story is the newest part of a decades-long battle to try and keep doctors from harming their patients by doing too much. Saini asks, how can we begin to advocate for a patient-centered approach based on evidence, when all other forces are pushing cardiologists toward surgical interventions?
Read Saini’s piece published in Health Affairs here, and see a longer version of the remarks below, which includes additional historical and political context. You can read Brownlee’s piece in Health Affairs at this link.
The remarkable results of the ORBITA trial raise two important questions about how we practice medicine: what is our scientific paradigm to evaluate what works and who decides what matters to patients? In cardiology, a decades-long process of re-evaluation has been in progress ever since the defibrillator first enabled the massive expansion of cardiac surgery.
In 1977 when Bernard Lown, whose team had developed the first usable defibrillator in 1962 and who had pioneered the coronary care unit at Harvard, felt forced to start managing patients without a coronary angiogram to avoid the reflexive urge of the house staff and other attendings (they kept scaring his patients into surgery), he began to wake up in the middle of the night worried that someone would drop dead and he’d be run out of Harvard and out of the practice of medicine.
Lucky for him that didn’t happen. Instead he and his group, which I joined in 1984 as a fellow and then as an attending, went on to develop a methodical, meticulous approach to stable coronary artery disease that emphasized medical treatment, diet, exercise, risk factor management, and most importantly, attention to the role of psychological stresses in the patients life.
Their first paper on a series of 212 patients was initially rejected by the New England Journal of Medicine, then published after Lown complained publicly to the editor, Bud Relman, at a cocktail party. The study showed remarkably low mortality using their noninvasive approach.
There was incredulity from the cardiology mainstream. There were criticisms: that it was not randomized, that not all had the coronary angiograms to prove that they had the disease, and that the patient population was highly selected – all valid points , but also, in 1981, completely beside the point. A biological possibility, like Roger Bannister running the 4 minute mile in 1954, had been demonstrated.
Over the next 20 years, as word leaked out around Boston and literally all over the world, we developed probably the deepest and longest experience anywhere of what is now called optimal medical therapy. We saw hundreds of 2nd opinion patients who had been told they needed surgery or stenting. Many even had an OR date scheduled. We managed 85% of them medically. They did well. We now have [currently unpublished] 12 year outcomes confirming those results. Furthermore, our analysis also suggests that the Appropriate Use Criteria developed in recent years by the cardiology professional societies to address this long-standing controversy are probably still insufficiently sharp an instrument to discern which patients are most likely to benefit from mechanical revascularization.
What has now become, cumulatively over many decades, a nearly trillion dollar question is this: how is it that such a heretical approach is conceived and executed, then ignored?
In the world of health care reform, it is now common to talk about “positive deviants”, i.e. out-of-the-mainstream examples of good clinical practice that ought to scale. Positive deviants should play a critical role in generating hypotheses by offering counter-narratives about what works. They also point to the risks of fetishizing randomized clinical trials in a situation where only the largest financial interests and the groupthink of the peer-review process can organize and conduct such trials.
That’s partly why old worldviews are so sticky. It took 25 years after Lown’s publication for the cardiology community to see the results of the COURAGE trial, which finally tested the value of stenting. It took another 10 years for the results of ORBITA to remind us that distorted worldviews can persist interminably.
Those results also remind us that another world is possible.
All of us therefore need to understand how such deviants arise in the first place, and then how to encourage them, embrace them and scale them up. At its core, the answer is that positive deviants arise out of the invention of an alternative approach powered by a alternative worldview.
Last week when I told Dr. Lown, who just turned 97, about this meeting, he had this to say:
“The situation is not futile, but advancing age brings great sobriety: it’s hard to influence a social enterprise like health when powerful economic interests are pushing in the opposite direction. If you can grapple with that, you can affect real social change.”
And make no mistake about it, this is not about one study or one paper. This is about changing social relationships. All you have to do is spend a few minutes on Twitter if you want to see the harsh thalamic reality of medical politics behind the masks of high mindedness.
If the results of the COURAGE trial, the first decent-sized RCT of stents vs medical management, were unsurprising to us at Lown, ORBITA on the other hand was at first glance astonishing. “Stents don’t work?” was the title we gave to the panel on ORBITA at our annual conference this year.
But upon reflection, we overreacted, and it seems to me that many people have been missing the forest for the trees. What’s been lost in the debate, ironically, is the remarkable power of medical therapy, underestimated for decades, driven by a mechanistic paradigm.
What’s been lost in the debate, ironically, is the remarkable power of medical therapy, underestimated for decades, driven by a mechanistic paradigm.
The initial astonishment at ORBITA’s results had been colored by the implicit, perhaps even unconscious comparisons to trials of medications where the control group consisted of people who are completely untreated. However, in ORBITA stenting was not compared to such a group; instead the control patient was treated with maximal medical therapy.
This confusion is understandable because the defined endpoint for ORBITA was explicitly derived from trials of medical therapy against no treatment. What the ORBITA team said was that since medical therapy in prior trials significantly improved exercise tolerance by nearly a minute in untreated patients, trying to detect a mere half a minute improvement with stenting seems really fair and reasonable. The logic (driven by the high confidence that stents are such powerful therapy) was that 30 seconds would be more than enough in patients, even those well-treated with medications.
Let’s be clear: ORBITA does not show that stenting is no better than sham for improving exercise tolerance – what it does show is that stenting is no better than sham for improving exercise tolerance in patients who have been optimized on medical therapy.
A more precise interpretation of the results therefore might be that compared to a completely untreated patient, optimal medical therapy has already captured most of the “therapeutic opportunity” for symptom relief. Beyond that, stenting is left without much more to add in most patients.
I think it’s important that we get this right and not overextrapolate. ORBITA has not disproven the idea that narrowing of the epicardial arteries of the heart can cause angina. Stenting did result in significantly more freedom from angina in the study.
What it has shown is that persistent narrowing of a coronary artery is not by itself a sufficient cause for function-limiting angina. But most cardiologists knew that already, or should have. We can have angina without blockage. We can have blockage without angina. Sometimes angina can remit almost completely on a good medical program.
I suspect that with a large enough sample, one might well be able to show that stenting has an incremental benefit on exercise tolerance. But so what? For whom would that be of value? The answer is: only for a subset of patients of unknown size, probably much smaller than most have assumed.
ORBITA reminds us to ask about the context and purpose of therapy – are we seeking the abolition of symptoms or enough control to achieve a functional life? That depends on whether we are treating a 60 year old hard-charging business executive or an 85 year old grandma who goes for a short, slow walk every day.
We know that most people do not get an adequate trial of medical therapy. The reasons are many. Most cardiologists are not trained to do it with anything like the rigor we practiced under Dr. Lown’s tutelage. Moreover, when one’s worldview is skewed by the dominant paradigm, in which the “real” cause is the blockage and medications are merely “bandaids,” there is an understandable itchiness to get on with the “cure.” That is conveyed to the patient, the nursing staff, primary care physicians and everyone else in a myriad of ways.
Heart disease is a well-known killer, but Dr. Lown was fond of saying, after his mentor Dr Samuel Levine: “Angina pectoris is a benign condition.”
That simple, provocative, counterintuitive statement conjures an entirely different worldview from that of, say, Eugene Braunwald, also at the Brigham, and a dominant figure in American cardiology, who would tell his trainees that you couldn’t manage CAD competently without defining the anatomy with an angiogram.
And it is that difference in worldview that allowed the positively deviant practice of the Lown Cardiovascular Group. Like the Catholic doctrine of a preferential option for the poor, we need to cultivate an unconflicted bias in favor of the patient. The whole patient.
One very simple example: exercise tolerance testing. At the Lown lab our central goal was to assess the patient’s overall fitness and functional status using the treadmill, with the presence of angina or rhythm disturbances being critical, but secondary.
We did not stop the test for changes in the EKG, even if profound, nor for the mere presence of angina. Angina only stopped the test when, either due to the intensity of discomfort, or to changes in blood pressure, the patient had to stop. Of course to do this safely required intense scrutiny during the test, high vigilance, and (at least so it seemed to a young cardiology fellow) nerves of steel.
This focus on the patient allowed us to better discriminate who would benefit from an invasive intervention. Call it holistic stress testing. Is that unscientific? No. It addressed the prime directive – when practicing medicine, don’t treat the number. Assess the whole person and that person’s life.
Our task now as a society is to forge such a new worldview, a new paradigm throughout health care, one in which we’re going to need a different kind of doctor and a different kind of science.
As Dr. David Brown has cited Thomas Kuhn, let me cite his predecessor, the German philosopher Georg Hegel. To get to a new paradigm, we need to aufhebung – to abolish, preserve and transcend, all at the same time — the old way of thinking. Central to that aufhebung is the need to transcend the pathological reductionism of our time. In other words, we need to bring the era of Flexner and Osler to a close and replace it with 21st century science.
Did you know that you can build a whole scientific career on one molecule? And since there are almost an infinite number of molecules in the human body, there are infinite career opportunities, as well as infinite opportunities for monetization. The slogan in Kendall Square, Cambridge could easily be: A company for every molecule and a molecule for every company!
This problem runs so deep that even if the United States were to get to single-payer coverage, this work would remain, because without it, all those dancing molecules and their noisy PR promoters will bankrupt the nation.
But beyond a scientific revolution we’re also going to need a new social paradigm.
That paradigm is almost certainly going to require a redistribution of power to patients and communities, so they can get the scientific information they need and decide for themselves what matters most. What ORBITA reminds us is that patient preferences matter a lot in defining the right care. If the scientific enterprise cannot account for that need, it will soon become morally bankrupt.
There are many specific policy ideas that can help us get there – too many to enumerate here — but it’s going to be a long road.
There is incredibly good news however.
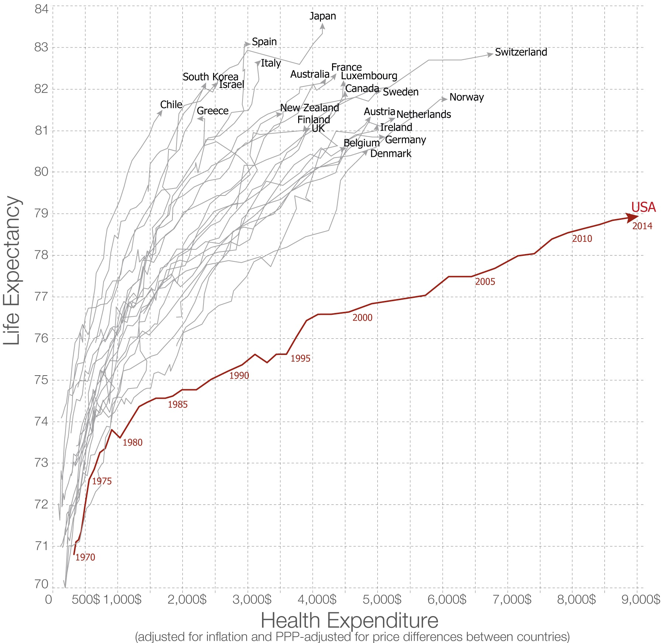
And this graph on the right is the proof. It’s a commonplace to point out that the US is a massive outlier among the OECD countries when it comes to healthcare spending. But what is less well-known is that our rogue status only emerged in the late 1970’s. In other words, the fault is not in our stars, nor in the air nor the water, nor in our DNA. Instead the graph shows that our current predicament is the tail end of a massive policy experiment.
And the results are in. We can debate the mechanisms, but reliance on the “magic of the market place,” as reflected in a series of policies adopted in the late 1970’s and early 80’s, has failed miserably in health care. This graph of paying more and more for less and less shows the sad result of the rent-seeking and wealth extraction that has come to dominate the American healthcare system today. It’s time for new thinking.