More than 1 in 10 veterans receive low-value care in the VA health system
Low-value care, also known as overuse, refers to medical services that offer little to no clinical benefit for patients. Not only do these unnecessary services waste billions of dollars, they also expose patients to the risk of physical, social, and financial harm.
For example, during the first year of Covid-19, about 100,000 older Americans were brought to the hospital for unnecessary procedures like stents, spinal fusions, and hysterectomies. From June to December 2020–when there were no vaccines available to vulnerable older adults–hospitals still delivered low-value procedures to Medicare patients at rates similar to 2019.
See the hospitals that do best on avoiding overuse for Medicare patients in your state!
Hospital overuse is ubiquitous in the US, particularly among older patients who have more interactions with the healthcare system. Research from the Lown Index published in JAMA Network Open last year found that more than a quarter of Medicare patients that came to the hospital for fainting were given unnecessary head imaging and 11% received unnecessary carotid artery imaging. Additionally, more than 20% of the spinal fusions and stents delivered in hospitals met criteria for overuse, along with 65% of hysterectomies.
What about overuse in the VA?
Research from the Lown Hospitals Index shows how prevalent overuse can be for Medicare patients. But what about the 9 million veterans who receive care at Veteran’s Health Administration (VA) hospitals and outpatient facilities?
The VA has unique features that make low-value care in the system worth studying. Unlike providers in the Medicare fee-for-service or Medicaid systems, VA providers are paid salaries rather than reimbursed for each service provided, giving them less of an incentive to deliver unnecessary tests and procedures. Additionally, VA providers are well-protected from malpractice lawsuits, so these doctors are under less pressure to perform low-value services defensively.
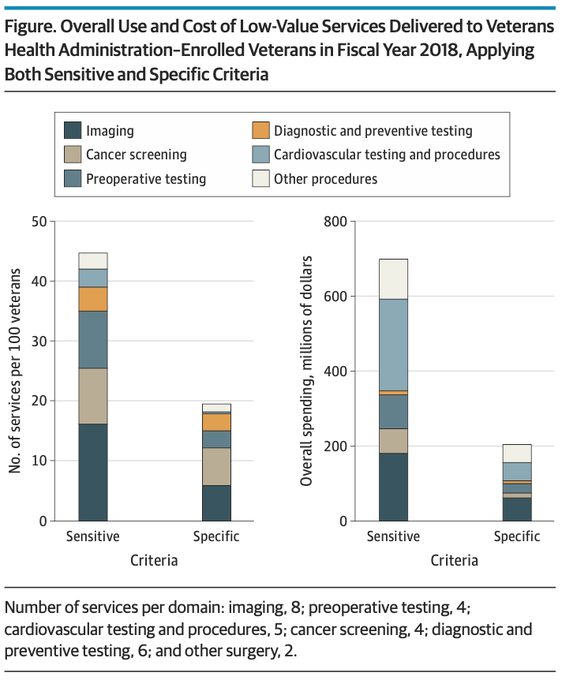
However, that does not mean that the VA is immune from overuse, a new analysis in JAMA Internal Medicine shows. Researchers at the Center for Health Equity Research and Promotion in the VA Pittsburgh Healthcare System examined the prevalence of 29 low-value tests and procedures in the VA in 2018. The low-value services studies included unnecessary cancer screening, diagnostic and preoperative testing, imaging, and cardiovascular procedures. They found that about 14% of veterans were exposed to at least one low-value service, at a cost of $206 million to the system.
And that’s the lower bound estimate. When researchers used broader criteria for the low-value services, the rate at which veterans were subject to low-value care doubled, and the cost of these services more than tripled.
The rate of overuse in the VA varied greatly depending on the type of service. Screening and testing were more prevalent than low-value procedures, likely because there is less perceived harm. Many doctors perform tests and imaging “just to be safe,” despite the very real risk of cascade events — follow-up tests, biopsies, and procedures that can lead to psychological and physical harm. For example, a whopping 99% of VA facilities performed prostate cancer screening tests for men 75 and older, for whom this screening is not recommended.
However, the most costly low-value services in terms of money were procedures. Spinal injections for low-back pain cost the VA system $44 million and stents for stable heart disease cost $37 million in 2018.
Reducing overuse throughout the system
These results provide valuable guidance to providers and administrators, showing them areas to focus on to reduce cost and harm from overuse in the VA system. More broadly, this study shows that physician salaries and global budgets are not a cure-all for overuse. While aligning physician incentives toward value is important, we also need to challenge the prevalent “more is better” culture in medicine to meaningfully reduce overuse.
Patient incentives need to align with high-value care as well. In an interview for the New England Journal of Medicine, Lown president Dr. Vikas Saini argued that we need economic incentives for patients and communities as well as doctors to reduce overuse. “If we reduce low-value care, the money doesn’t go back to communities to invest in health. If you don’t have parties who can clearly see how they gain, they’re not motivated,” he said.
“The challenge is that overuse is a systemic problem. It needs systemic solutions.”
Vikas Saini, New England Journal of Medicine
On the other hand, ensuring that patients are engaged and trust their clinicians may help reduce overuse. As our late founder Dr. Bernard Lown wrote, “Fully informed patients, trusting their physicians, do not insist on tests or procedures.”